Reservar cita
Medical Repatriation in Latin America: How Cases Actually Work
 Por
Por
Medical repatriation is one of the more operationally demanding services an assistance company, insurer, or carrier coordinates. A member is abroad, clinically fragile, and the clock is running on both the clinical picture and the cost. This guide sets out what medical repatriation is, when a case is triggered, how repatriation and evacuation insurance pay for it, and how a case is actually run on the ground in Latin America: the intake, the medical clearance, the transport, and the land side at each end. It is written for the desks that manage these files: travel-assistance companies, third party administrators (TPAs), travel-medical and IPMI (international private medical insurance) insurers, and aeromedical operators.
What is medical repatriation?
Medical repatriation is the organized return of a patient to their home country, or their home physician, after a medical event or planned treatment abroad. It is carried out with the level of medical support the patient’s condition requires in transit. That definition is what separates it from medical evacuation. Evacuation moves a patient experiencing an emergency to the nearest facility that can treat them; repatriation moves a stabilized patient home once they can tolerate the longer journey (Centers for Disease Control and Prevention (CDC) Yellow Book). The two often sit on the same file at different stages: an evacuation to stabilize the patient locally, then a repatriation home once they are fit to travel.

The level of support scales with the case. A stable patient may fly commercially with a medical escort; a more acute case may need a stretcher, in-flight oxygen, or a dedicated air ambulance. Deciding which is a clinical judgment, not a booking preference, and it is documented before anyone travels.
When is a repatriation case triggered?
A repatriation is triggered when a patient is stable enough to move but still needs to get home, either for continuing care or because the episode abroad is finished. In practice the trigger is one of a few recurring situations:
- Hospitalized abroad, now stable: a traveler or expat has been admitted overseas and is well enough to move home for ongoing treatment or recovery.
- A planned procedure is complete: a cross-border surgical or medical case is done and the patient has been cleared to return.
- The payer wants care continued at home: a home insurer or employer wants the member’s care resumed in-network once they are stable, rather than run an open-ended stay abroad.
Who sets the case in motion varies. It may be the travel-assistance company acting for the insurer, the travel-medical or repatriation insurer directly, the treating hospital that wants a bed back, or the family. Whoever opens the file, the coordinating desk owns it from that point: confirming coverage, arranging clearance, and booking the transport.
How do medical repatriation insurance and evacuation cover it?
Repatriation is almost always paid through insurance rather than out of pocket, but the exact benefit depends on the policy. Medical repatriation insurance, sold on its own or bundled with evacuation cover as medical evacuation and repatriation insurance, is held by international travelers, expatriates, corporate global-mobility programs, and IPMI members. Coverage terms, limits, exclusions, and pre-authorization rules vary by carrier and product, so this guide does not state them as fact. The policy governs, and the assistance desk confirms them case by case.
What is consistent across cases is the paperwork that authorizes and enables the move. Two documents run a repatriation:
- The Guarantee of Payment (GOP): a formal authorization the insurer or assistance provider issues directly to the treating hospital so care and transport can proceed without delay, while the carrier keeps the right to determine final coverage later against the policy terms (Aetna International Guarantee of Payment guide). It is an access mechanism, not a final claim decision.
- The MEDIF (medical information form): the International Air Transport Association (IATA)-standard form the treating physician completes to clear the patient as fit to fly and to specify the support needed in transit, such as oxygen, a stretcher, or a medical escort (IATA MEDIF form). Passenger medical clearance for air travel sits within IATA’s medical framework for carrying sick passengers (IATA Medical Manual).
The GOP unlocks the money; the MEDIF unlocks the seat. A case does not move until both are in hand, which is why coordination, not transport, is usually the slow step.
Because the benefit is paid against the policy, the case has to be costed in full and documented as it runs. That means not only the flight, but the medical escort or air-ambulance charge, ground ambulance at both ends, any overnight lodging for the patient or an accompanying family member, and the in-country coordination itself. A repatriation billed as a single transport line rarely survives a payer’s review; an itemized file that maps back to the GOP does.
What does a repatriation case involve on the ground?
The core sequence of a repatriation is the same regardless of who holds the policy, and it determines whether a case runs clean or stalls. This is where MTP fits: it is the in-country logistics and assistance layer, not the insurer or the carrier. A single case runs through these stages:
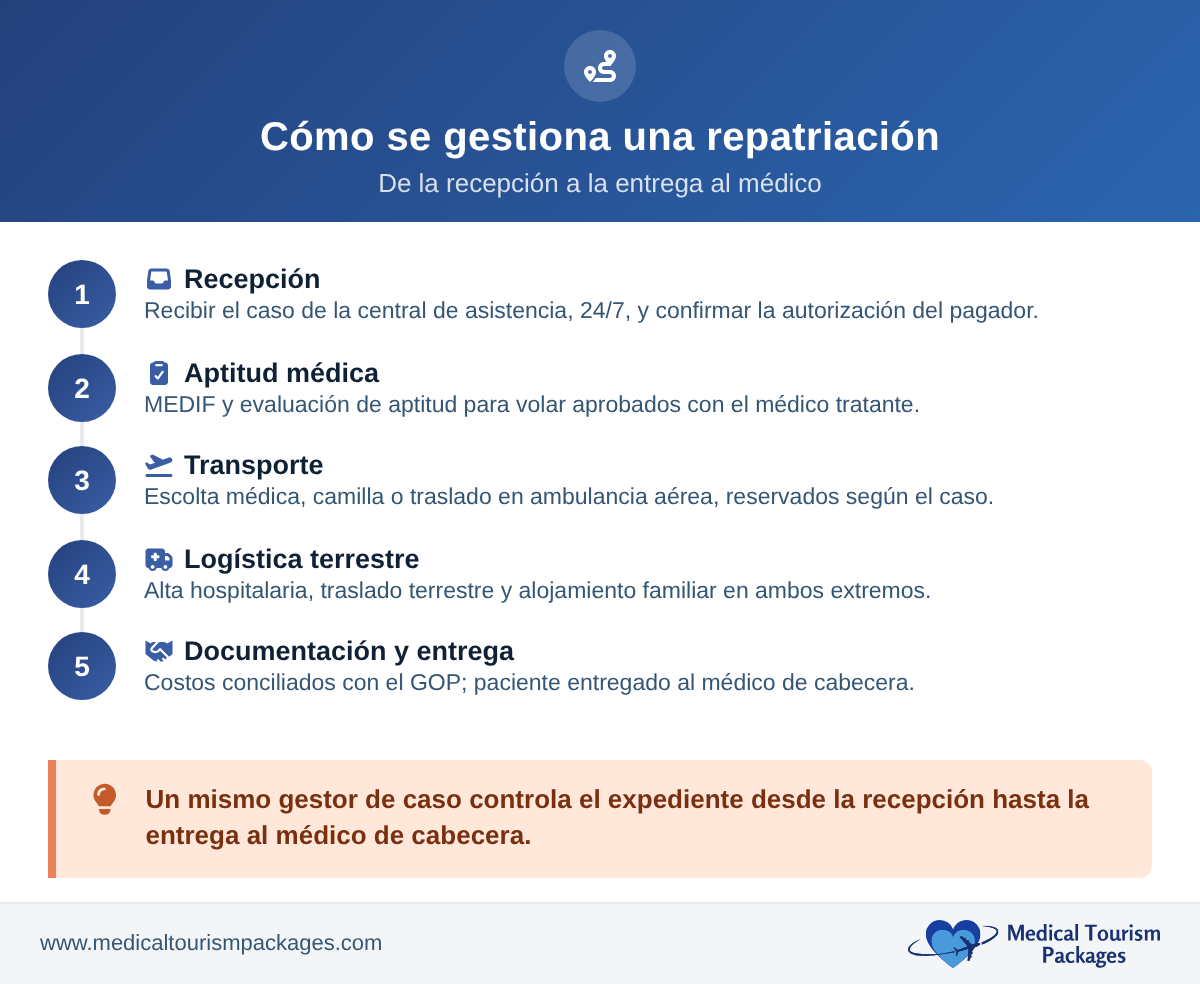
- Intake: receiving and reviewing the file from the assistance desk, on a 24/7 basis, and confirming what the payer has authorized.
- Medical clearance: coordinating the MEDIF and fit-to-fly assessment with the treating physician, and confirming the support level the patient needs in transit.
- Transport: arranging the move itself, whether a commercial medical escort, a stretcher booking, or the handoff to an air-ambulance operator, plus the land side at both ends: hospital discharge, ground ambulance or transfer, and family lodging where needed.
- Documentation: reconciling costs and billing against the GOP so the case matches what was authorized.
- Handoff: delivering the patient to the home physician or receiving facility so care continues without a gap.
Every one of these steps generates a document, a time stamp, and a cost line. Keeping them itemized and reconciled to the GOP is what makes the case defensible to the payer afterward.
Cases stall in predictable places. Medical clearance slips when the MEDIF and the latest treating-physician report do not arrive together, or arrive too close to departure for the carrier’s medical desk to sign off in time. The land side slips when a discharge is booked without a confirmed ground transfer, or when lodging for an accompanying family member was never authorized. Naming those gaps at intake, rather than at the airport, is most of what a coordinating desk is paid to do.
How does repatriation work across Colombia, Panama, Costa Rica, and Mexico?
MTP runs the land side of these cases with local teams in Bogotá, Panama City, San José, and Mexico City, so the discharge, ground transport, lodging, and airport logistics are handled by people who work in the destination rather than remotely. One case manager owns the file end to end, which gives the assistance desk a single point of contact from intake through the home handoff.
For return logistics, Panama and Mexico carry a practical advantage: their proximity and dense air links to the United States shorten routing and widen the options for a commercial escort or air-ambulance transfer to a US receiving facility. The full engagement model for assistance companies, insurers, and carriers is set out on our patient logistics partner page.
How do repatriation and cross-border claims connect?
A repatriation does not end when the patient lands. Every case generates a claim that has to be documented to the payer’s standard. The GOP, the itemized transport and facility costs, the clinical records, and the clearance paperwork all have to reconcile before the file closes. How a TPA then adjudicates and passes those cross-border claims through is its own subject, covered in our companion guide on TPAs and cross-border claims.
Sources
- Medical evacuation vs. repatriation (evacuation to the nearest capable facility; repatriation home once stabilized): CDC Yellow Book: Travel Insurance and Medical Evacuation Insurance.
- Guarantee of Payment (GOP) definition and function: Aetna International Guarantee of Payment guide.
- MEDIF (Medical Information Form) for air travel: IATA MEDIF form.
- Passenger medical clearance framework: IATA Medical Manual.
Coordinate a repatriation case
Running a repatriation case in Latin America? We are the in-country fulfillment arm for assistance companies, insurers, and carriers, with a single case manager per file and GOP and MEDIF workflows as standard.